

Achieving quality assurance in laboratories in rural Zambia
Saint Francis Hospital (SFH) (Figure 1) is 1 of 2 referral hospitals serving more than 1.5 million people, most of whom live in subsistence farming communities in Zambia’s Eastern Province. We wanted to improve quality assurance in the laboratory service at SFH. The first step was to ensure that all laboratory staff were committed to implementing a quality management system with the ultimate aim of achieving formal accreditation.1 To achieve our goals, we established collaborations with the 3 institutions listed in Table 1.

Collaborating institutions and services provided to SFH
| Institution | Location | Nature of collaboration |
|---|---|---|
| University Teaching Hospital | Lusaka, Zambia | • Reporting of BM aspirate by qualified pathologist • Liaison with physicians for transfer of patients with hematologic malignancies • 2-week site visit, audit, and training by 2 quality experts, with technical support in implementing the Quality Management System |
| Chipata Central Hospital | Chipata, Zambia | • Exchange program for blood samples • Two-way technical support |
| Royal Prince Alfred Hospital | Sydney, Australia | • Provide general guidance for producing laboratory manuals • Furnish a quality manager to provide technical assistance on-site for 2 weeks (September 2019) |
| Institution | Location | Nature of collaboration |
|---|---|---|
| University Teaching Hospital | Lusaka, Zambia | • Reporting of BM aspirate by qualified pathologist • Liaison with physicians for transfer of patients with hematologic malignancies • 2-week site visit, audit, and training by 2 quality experts, with technical support in implementing the Quality Management System |
| Chipata Central Hospital | Chipata, Zambia | • Exchange program for blood samples • Two-way technical support |
| Royal Prince Alfred Hospital | Sydney, Australia | • Provide general guidance for producing laboratory manuals • Furnish a quality manager to provide technical assistance on-site for 2 weeks (September 2019) |
Engaging and motivating staff
A major challenge in resource-poor settings is staff morale.2 To motivate staff, we conducted presentations and meetings that covered a variety of topics such as defining requirements for quality in performing laboratory procedures and in completing tasks, instituting formal handover, setting goals, reviewing the roster (which resulted in staff working 1 weekend every 2 weeks rather than every weekend), holding laboratory meetings on a weekly rather than a monthly basis, and fostering a safe environment for learning.
Participating in a national quality improvement program
Through networking, a meeting was arranged with the National Coordinator for Laboratory Services in Zambia. The meeting resulted in a plan for the laboratory to be formally audited and for catch-up workshops to be held. This allowed SFH to become part of the existing national program already in place—Strengthening Laboratory Management Toward Accreditation—which staff were previously not aware of.
Collecting and labeling samples
Poor specimen labeling has been a problem at SFH (Figure 2). A policy was instituted specifying that at least 3 identifiers are required for each specimen: patient’s name, date the sample was taken, and hospital record number (HRN) or date of birth (DOB). This requirement was communicated to clinicians at hospital and departmental meetings over a 1-month period. Labeling of EDTA tubes was audited in the hematology laboratory at the start of the intervention and again 5 months later. All the tubes that had been tested at the end of Monday and Tuesday of a predetermined week were examined. Differences were evaluated by using Pearson’s χ2 test (Table 2). Although there was no further intervention, the results showed a marked and statistically significant improvement in labeling practice.

Poor labeling practice. An anticoagulant-coated specimen tube with no patient details on its label was sent out with a request for blood count analysis.
Poor labeling practice. An anticoagulant-coated specimen tube with no patient details on its label was sent out with a request for blood count analysis.
Characteristics of blood tube labeling before and after educational intervention
| Label | Before intervention (n = 57) | After intervention (n = 64) | χ2P | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Labeled with HRN or DOB | 3 | 5.3 | 11 | 17.2 | <.001 |
| Labeled with date | 24 | 42.1 | 34 | 53.1 | .23 |
| 3 identifiers (name, date, and HRN or DOB) | 5 | 8.8 | 16 | 25 | .02 |
| Label | Before intervention (n = 57) | After intervention (n = 64) | χ2P | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Labeled with HRN or DOB | 3 | 5.3 | 11 | 17.2 | <.001 |
| Labeled with date | 24 | 42.1 | 34 | 53.1 | .23 |
| 3 identifiers (name, date, and HRN or DOB) | 5 | 8.8 | 16 | 25 | .02 |
DOB, date of birth; HRN, hospital record number.
Standardizing blood film staining
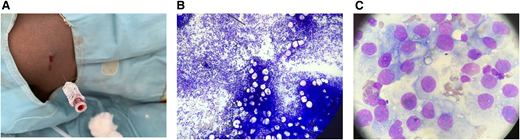
The majority of blood films (BFs) were previously characterized by poor uptake of basophilic dye which resulted in unsatisfactory staining of white blood cells making them unidentifiable (Figure 3A). The BFs were also subjected to poor smear techniques and water artifacts. BF tracking was not possible because of inadequate labeling, absence of accession numbers, and lack of storage. Several weeks’ worth of troubleshooting resulted in a new standard operating procedure (SOP) that was designed specifically for our laboratory, and it included improved staining procedures (Figure 3B-C) that were incorporated into a comprehensive Microscopy Manual. Previously, BF staining showed significant variation in staff technique and practice because there was no SOP. Because previous BFs had not been stored, a formal comparison between previous BFs with those from current practice was not possible. Review of the most recent group of stored slides (from May and part of June 2019) showed satisfactory staining in 42 of 42 slides.

Stained sample slides and staining procedures. (A) The staining process failed because of poor uptake of basophilic dye by white blood cells. (B) Laboratory staff assessing a variety of staining protocols. (C) Successful staining of a lymphocyte (the pediatric patient was unexpectedly found to have falciparum malaria).
Stained sample slides and staining procedures. (A) The staining process failed because of poor uptake of basophilic dye by white blood cells. (B) Laboratory staff assessing a variety of staining protocols. (C) Successful staining of a lymphocyte (the pediatric patient was unexpectedly found to have falciparum malaria).
Introducing a new BF morphology service
BF examination is one of the most important tests in resource-poor settings.2 With improved stains and better staining procedures, our main limitation then became interpreting the slides. Staff had little training in cell morphology other than that for malaria and sickle cell disease (Figure 4). Blasts and schistocytes were not being correctly identified, which is vital for diagnosis of leukemia and microangiopathy. We initiated a teaching program (still ongoing) so that hematologic and other disorders could be correctly diagnosed, which would allow patients with conditions such as acute leukemia to be appropriately referred for treatment.

We conducted an audit to compare the rates of diagnosis of hematologic malignancies 14 weeks before and 14 weeks after implementation of qualified BF reporting (a qualified morphologist was on-site during this period). The hospital record system was searched for diagnoses using the search terms “leukaemia”, “blood cancer”, “hematologic malignancy/cancer”, and “lymphoma”, and patient files were reviewed. The laboratory BF record for the same period was also searched, and files for additional patients were obtained. A χ2 test was applied to the combined results (Table 3), which showed a statistically significant increase in diagnosis of leukemias (P = .005). External quality assurance is being arranged to ensure that staff maintain competency once their training is complete.
Hematologic malignancies diagnosed on BFs at SFH before and after intervention
| Hematologic disorder | 14 weeks before intervention (n = 3954 admissions) | 14 weeks after intervention (n = 5052 admissions) | P |
|---|---|---|---|
| Acute leukemia | 0 | 6 | |
| Other myeloid leukemia | 0 | 2* | |
| Leukemic lymphoproliferative disorder | 0 | 2 | |
| Any leukemia | 0 | 10 | .005 |
| Any hematologic malignancy | 1† | 10 | .02 |
| Hematologic disorder | 14 weeks before intervention (n = 3954 admissions) | 14 weeks after intervention (n = 5052 admissions) | P |
|---|---|---|---|
| Acute leukemia | 0 | 6 | |
| Other myeloid leukemia | 0 | 2* | |
| Leukemic lymphoproliferative disorder | 0 | 2 | |
| Any leukemia | 0 | 10 | .005 |
| Any hematologic malignancy | 1† | 10 | .02 |
These cases were chronic myelogenous leukemia (CML) and a suspected case of atypical CML.
This case was the result of a lymph node biopsy documented by clinicians, although the report was not found in the file.
Improving malaria detection
An SOP for analyzing thick films was devised on the basis of the malaria vertical program in Zambia and was incorporated into the Microscopy Manual. We observed that staff were reporting the results of malaria thick films after as little as a few seconds of observation. After a missed diagnosis occurred, a minimum observation time of 5 minutes by a competent microscopist with confirmation by a second observer is now required. We introduced mandatory thin films as part of the assessment, which is important for speciation (Figure 3C).
Using BM biopsies for diagnosis and referral
The University Teaching Hospital (UTH) in Lusaka (the capital) is Zambia’s main referral hospital. In the provinces, expertise in hematology is lacking. Definitive diagnosis for hematologic disorders is made in Lusaka and requires that patients be transferred there for further investigation. This is very expensive for families who must bear the costs of travel and lodging. Thus, patients often deteriorate and die without any meaningful intervention. UTH staff have now trained workers at 3 of the 9 provincial hospitals to perform bone marrow (BM) biopsies and form preliminary opinions on peripheral BF and BM aspirate smears. This resulted in clinical staff sending only peripheral BF or BM smears to Lusaka rather than sending the patients themselves. As a result, patients have a more definitive diagnosis at the time of referral for treatment, and referrals for conditions that can be managed locally (eg, megaloblastic anemia) have been avoided.
Introducing BM aspiration service
Similarly, BM aspiration was introduced to SFH in carefully selected patients to allow diagnosis and avoid the need to transfer patients to Lusaka (6 of 6 BM aspirations were successful; Table 4). Because resources are limited, we used spinal needles as described in the literature3 (Figure 5A). A clinician is currently being trained in the technique, and laboratory staff will prepare slides that can then be sent to UTH for reporting (Figure 5B-C). By the time the current morphologist leaves, procedures will be in place to ensure that BM aspirates can continue to be taken and will continue to be reported to UTH as described above.
BM aspirate results to date at SFH
| BM aspirate No. | Diagnosis |
|---|---|
| 1 | Immune thrombocytopenia |
| 2 | Extrapulmonary tuberculosis |
| 3 | Agranulocytosis |
| 4 | Likely peripheral cause of cytopenia (tropical splenomegaly syndrome) |
| 5 | Morphologic dysplasia, diagnosis uncertain |
| 6 | Malignancy, suspected metastatic disease |
| BM aspirate No. | Diagnosis |
|---|---|
| 1 | Immune thrombocytopenia |
| 2 | Extrapulmonary tuberculosis |
| 3 | Agranulocytosis |
| 4 | Likely peripheral cause of cytopenia (tropical splenomegaly syndrome) |
| 5 | Morphologic dysplasia, diagnosis uncertain |
| 6 | Malignancy, suspected metastatic disease |
BM aspiration procedure and aspirates. (A) BM aspiration using a spinal needle. BM smear slides showing (B) BM aspirate from a spinal needle and (C) sixth successful BM aspirate with cells indicative of suspected metastatic disease.
BM aspiration procedure and aspirates. (A) BM aspiration using a spinal needle. BM smear slides showing (B) BM aspirate from a spinal needle and (C) sixth successful BM aspirate with cells indicative of suspected metastatic disease.
Managing patient transportation
It was realized soon after morphologic diagnoses of acute leukemia began that patients were not able to be treated because of lack of transportation to Lusaka, where the country’s only cancer treatment center is located (Figure 6). Therefore, an advocacy project was initiated to establish a fund that could be tapped into by the hospital when urgent transport is required and no funding is available. More than US$7000 has been raised from support in Australia, the United Kingdom, and Ireland.4

Most patients from the villages struggle to find the funds to transport themselves to Lusaka.
Most patients from the villages struggle to find the funds to transport themselves to Lusaka.
Performing QC for blood count analyzers
The rates of performing of quality control (QC) and preventive maintenance were low. So procedures were established that require daily QC; daily, weekly, and monthly preventive maintenance; and engineer servicing and documentation once every 6 months. A laboratory manual incorporating SOPs is also planned. A program for exchanging samples was arranged with the provincial Chipata Central Hospital Laboratory (Chipata, Zambia). Our laboratory staff were educated on the importance of performing QC. Data were collected retrospectively measuring documented QC completion in the hematology laboratory before the intervention (third quarter [Q3] and Q4 of 2018) and after the intervention (Q1 and Q2 until June 16, 2019) for blood count analyzers (Figure 7). Pearson’s χ2 test was applied to the data, and the result showed significant improvement in QC performance (P < .001) (Tables 5 and 6).
The importance of preventative maintenance and QC on the quality of laboratory results has been a point of focus at SFH. This photo shows our HORIBA ABX Micros 60 automated hematology analyzer used for in-vitro diagnostics testing of whole blood specimens.
The importance of preventative maintenance and QC on the quality of laboratory results has been a point of focus at SFH. This photo shows our HORIBA ABX Micros 60 automated hematology analyzer used for in-vitro diagnostics testing of whole blood specimens.
QC completion (days) before and after staff intervention
| Instrument | 2018 | 2019 | ||||||
|---|---|---|---|---|---|---|---|---|
| Q3 (92 days) | Q4 (92 days) | Q1 (90 days) | Q2 (to June 16) (81 days) | |||||
| No. | % | No. | % | No. | % | No. | % | |
| Micros 60 | 24 | 26 | 9 | 10 | 49 | 54 | 37 | 48 |
| Sysmex XN-550 | 19 | 21 | 12 | 13 | 37 | 41 | 49 | 64 |
| Instrument | 2018 | 2019 | ||||||
|---|---|---|---|---|---|---|---|---|
| Q3 (92 days) | Q4 (92 days) | Q1 (90 days) | Q2 (to June 16) (81 days) | |||||
| No. | % | No. | % | No. | % | No. | % | |
| Micros 60 | 24 | 26 | 9 | 10 | 49 | 54 | 37 | 48 |
| Sysmex XN-550 | 19 | 21 | 12 | 13 | 37 | 41 | 49 | 64 |
Documented performance of daily QC for blood count analyzers before and after staff intervention
| Instrument | Before intervention (%) (Q3 + Q4 2018) | After intervention (%) (Q1 + Q2 2019) | χ2P |
|---|---|---|---|
| Micros 60 | 18 | 51 | <.001 |
| Sysmex XN-550 | 17 | 51 | <.001 |
| Instrument | Before intervention (%) (Q3 + Q4 2018) | After intervention (%) (Q1 + Q2 2019) | χ2P |
|---|---|---|---|
| Micros 60 | 18 | 51 | <.001 |
| Sysmex XN-550 | 17 | 51 | <.001 |
Planning for a new coagulation monitoring service
Currently at SFH, patients with thrombotic disorders or cardiac arrhythmias cannot be treated adequately because of the inability to monitor warfarin therapy, and newer anticoagulants are too expensive. The majority of patients who need anticoagulation therapy are treated with aspirin. Warfarin is very inexpensive (about US$0.08 per tablet). The laboratory is currently investigating options to procure an instrument for coagulation testing to monitor patients receiving anticoagulation therapy (warfarin). Factors being assessed include instrument performance, upfront and ongoing costs, requirements for maintenance, space and energy consumption, effect of humidity, staff training, implementation of quality assurance, establishment of reference ranges, and the need for an SOP. International normalized ratio testing will allow use of warfarin instead of aspirin, which is relatively ineffective.
Looking ahead
There is still room for significant improvement in many of the aspects of the operation of our laboratory (eg, labeling of tubes, QC). However, the work performed to date shows that significant progress and quality improvement are achievable. We expect that, with the continuation of this trend, the laboratory will conform to ISO 15189 and achieve formal accreditation within the next 1 to 2 years.
Authorship
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Ahmad Alcheikh, Saint Francis Hospital, Private Bag 11, Katete, Zambia; e-mail: a.alcheikh@gmail.com.

